All students must keep a daily electronic log of required clinical experiences encountered during their clinical rotations. The log centers around required clinical experiences (a “must see list”) developed by the faculty and part of the course syllabus. This log is web-based and accessed through “the SGU portal” (details below). The log contains multiple fields that students must complete for each patient encounter: rotation, hospital, date, chief complaint, primary diagnosis, secondary diagnoses, clinical setting, communication course chapters, level of responsibility and category of illness. The log also has a form upload feature and an optional comment section. Students can use the form upload feature for required case write-ups and other required forms (ex. Direct observation form, Preventative FM Visit form) Once the forms are uploaded they are displayed on the student final evaluation for the Clerkship director to view. The optional comment section to note relevant cultural issues, documenting a SOAP note, procedures or medical literature relevant to the patient. We recommend that the log be kept current on a daily basis. This log serves multiple functions and, as discussed below, will be used in different ways and for different purposes by students, by the clinical faculty at affiliated hospitals and by the Office of the Dean. Students must remain HIPAA compliant by not using any patient identifiers, such as names, initials, date of birth, medical record numbers, pictures or other identifying information.
New Direct Observation Form for Feedback on Clinical Knowledge, Skills, and Professional
Behavior
- St. Georges University School of Medicine has approved a new direct observation requirement for all students starting core clerkships after May 2022 to provide students with formative feedback on their clinical knowledge, skills, and professional behavior
- Students must be observed by a clinical preceptor and provided with formative feedback on their performance during a clinical encounter.
- Students are responsible for notifying their preceptors to arrange the required direct observation.
- The preceptor must select an appropriate patient for the observed clinical encounter.
- The preceptor must complete the Direct Observation Form to provide immediate formative feedback on the selected clinical encounter.
- The Direct Observation Form may be completed during one or several clinical encounters. Each direct observation metric can be performed in small parts throughout the clerkship. This will decrease the time burden on preceptors.
- The student will upload the Direct Observation Form for display into the final evaluation for the Clerkship director to review. Details for uploading the form will be provided on the clerkship Sakai site.
- Completion of the Direct Observation feedback experience and uploading of the form are required for each clerkship. Failure to complete this requirement may negatively impact a student’s professional behavior component grade for the rotation.
The Faculty:
The Direct observation requirement has been developed to assess a student’s clerkship specific learning objectives during a patient encounter.
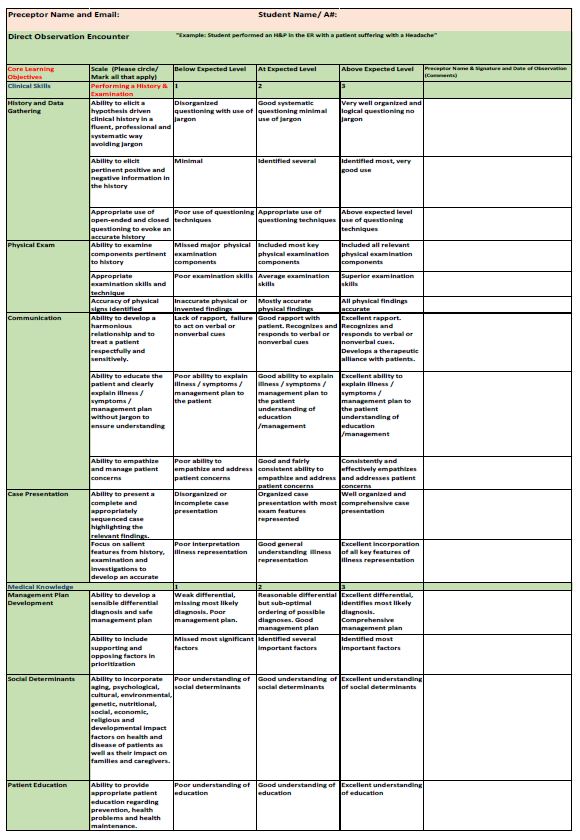
The Following learning objectives will be assessed:
- Medical Knowledge
- Clinical Skills
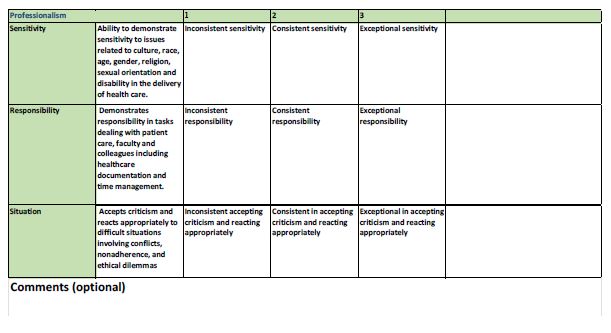
- Professional Behaviour
During the direct observation the preceptor will apply the defined scales on the direct observation form to assess SGU students in a clinical setting. Preceptors should follow the below instructions for an optimal learning experience:
- Together with the student, select an appropriate patient
- Inform the patient and ask permission
- Provide constructive feedback to student:
- Feedback is based on an assessment of the student’s knowledge, clinical skills and professional behavior observed during the direct observation of the clinical encounter.
- Give feedback as soon as possible, correct questioning and exam maneuvers in real time.
- Feedback should be constructive, consisting of a combination of positive and negative verbal/written comments with instructions for improvement.
- The entire form does not need to be completed all at once. This will ensure the direct observations will not burden preceptors with excessive time constraints.
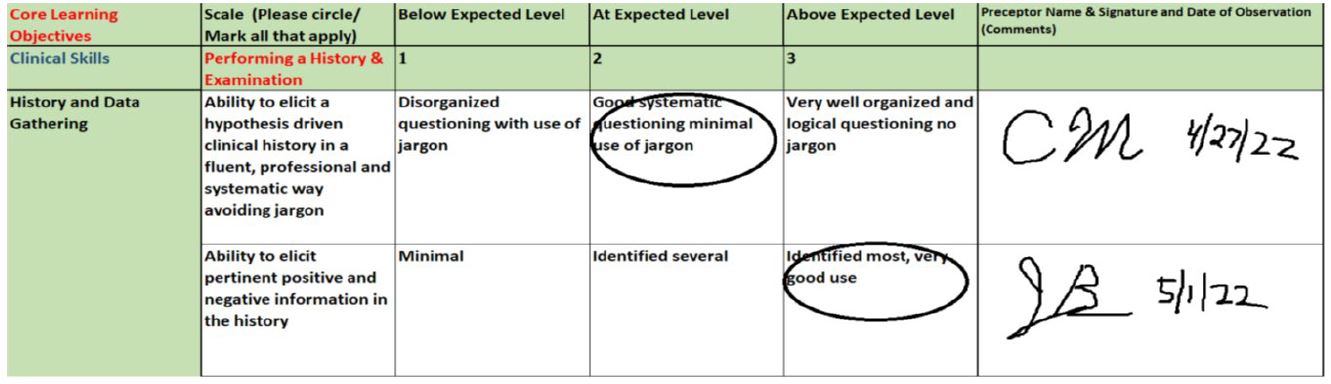
- Once the individual metric is observed please circle the appropriate skill level, sign and date in the comment section. (See below)
Students:
Students are to download and print the form found in Core Sakai Resources and have it present at all times during the rotation.
Students must coordinate with the preceptor to examine an appropriate patient.
The student must hand the preceptor the Direct observation form before the observation of the clinical encounter.
Once the clinical encounter is performed the student will receive verbal feedback on the observed metric and have the preceptor circle the appropriate skill level, sign and date the metric assessed. This may be done during different encounters with different preceptors until all metrics on the Direct Observation form have been observed and the feedback form has been completed.
Once the entire form has been completed the student will upload the Direct Observation form into PEL (upload feature) for display into the final evaluation system for the Clerkship director to review.
Pictures of the completed Direct observation form must be saved and uploaded in a JPEG format
Number of Direct Observations:
Internal Medicine and Surgery: (12-week rotations)
- Require 2 completed Direct Observation forms to be submitted by students. The first before the midcore evaluation for formative feedback and the second before the final evaluation.
Pediatrics, Psychiatry and Obstetrics & Gynecology:
- Require 1 completed Direct Observation form to be submitted by students.
Direct Observation Form:
Rationale for the patient encounter log
During the clinical years students need to develop the clinical competencies required for graduation and postgraduate training. These competencies are assessed in many different ways: by faculty observation during rotations, by communication skills assessments, by completion of web-based assignments and by NBME clinical subject exams. In order to develop many of these competencies and meet the objectives required for graduation, the school needs to ensure that each student sees enough patients and an appropriate mix of patients during their clinical terms. For these reasons, as well as others discussed, below the school has developed this log.
One of the competencies that students must develop during their clinical training involves documentation. Documentation is an essential and important feature of patient care and learning how and what to document is an important part of medical education. Keeping this log becomes a student training exercise in documentation. The seriousness and accuracy with which students maintain and update their patient log will be part of their assessment during the core rotations. In terms of the log, how will students be assessed? Not by the number of diagnoses they log, but by the conscientiousness and honesty they exhibit documenting their patient encounters. All of these features of documentation – seriousness, accuracy, conscientiousness and honesty – are measures of professional behavior.
Definition of a patient encounter
Students should log only an encounter with or exposure to a real patient. Simulated patients, case presentations, videos, grand rounds, written clinical vignettes, etc. should not be logged even though they are all important ways to learn clinical medicine. Many of these educational experiences, along with self-directed reading, are necessary preparation for USMLE Step 2 and postgraduate training. This log, however, focuses on a unique and critical component of clinical training, namely, involvement with “real” patients. Student involvement with patients can occur in various ways with different levels of student responsibility. The most “meaningful” learning experience involves the student in the initial history and physical exam and participation in diagnostic decision making and management. A less involved but still meaningful encounter can be seeing a patient presented by someone else at the bedside. Although the level of responsibility in this latter case is less, students should log the diagnoses seen in these clinical encounters. Patient experiences in the operating or delivery room should also be logged.
For students
- The lists of symptoms (chief complaints) and diagnoses serve as guidelines for the types of patients the clinical faculty think students should see over two years of clinical training. The clinical faculty feels that students should have clinical exposure to about 50 symptoms (chief complaints) and about 180 diagnostic entities. These lists can also serve as the basis for self-directed learning and independent study in two ways:
- If students see a patient and enter that patient’s primary and secondary diagnoses in the log, they will be expected to be more knowledgeable about these clinical entities and to do additional reading about them, including some research or review articles. If relevant, students can study and log a communication skills module.
- If, at the end of a clerkship or FM, students discover they have not seen some of the clinical entities on the required list during the core rotations, they can view the virtual links provided in Sakai and enter them in the log as a virtual encounter. Students are also told to see these required encounters in the fourth year.
- The different fields in the log should stimulate students to look for and document the complexities of clinical encounters when appropriate. Many patients present with multiple medical problems. For example, an elderly patient admitted with pneumonia (primary diagnosis) may also have chronic lung disease, hypertension and depression (secondary diagnoses). The patient may have fears about death that need to be discussed. We hope by keeping the log students will develop a more profound understanding of many patient encounters.
- Students may, and many times should, review and edit the log (see “Instructions to access and use the log” below). The original entry might require additions if, for example, a new diagnosis is discovered, the patient moves from the ED to the OR to the wards or a patient presenting with an acute condition deteriorates and presents end-of-life issues. These developments require a return to the original entry for editing.
- The chief complaint and diagnosis lists do not include every possible diagnosis or even every diagnostic entity students must learn about. The list reflects the common and typical clinical entities that the faculty feels SGU students should experience. The same list of diagnoses is presented in two ways - alphabetically and by specialty. Both lists contain the same diagnoses and students can use whichever one is easier. If students encounter a diagnosis not on the list, they should choose the most related diagnosis from the list. By looking at “standard” diagnoses, the school can monitor the overall clinical experiences students are having at different affiliated hospitals.
- Students must learn more than they will experience during clinical rotations. The log does not reflect the totality of the educational objectives during the core clerkships. Clinical experience is an important part, but only a part, of clerkship requirements. Students need to commit themselves to extensive reading and studying during the clinical years: “Read about patients you see and read about patients you don’t see”.
- The NBME Clinical Subject Exams at the end of the clerkship are not based on the log but on topics chosen by the NBME.
- We encourage students to maintain this log throughout their 80 weeks of clinical training. The University requires that the logs be formally evaluated only during the clerkships. However, the list reflects those entities the faculty thinks students should encounter during their entire clinical experience in medical school, not just during the clerkships. The Office of the Dean monitors student logs throughout the clinical terms to assure compliance with the required encounters.
Instructions to students for access and use of the Patient encounter log system
The link to the Patient Encounter Log is found in the SOM Clinical Studies section. Clicking on this Patient Encounter Log link will take you to the sign in and then the Main Menu. From this menu, you can perform the following actions:
- Enter a new patient encounter
- Review or Edit my encounter logs
When you select Enter a new patient encounter, you will see pull down selections for all of the fields except “Comments”. Make your selections and click Submit My Log. Entry in all of the fields is required.
The main menu selection Review or Edit your encounter logs will take you to a screen which lists all of your logs. Select the one you’d like to see or change. The Edit This Log button will allow you to make changes to the individual log.
If a printed copy is requested, Select print your logs from the menu to prepare a printer-friendly formatted table of your logs. Select the logs to include for printing and click Print Selected Logs. On the next page, click Print this Page to receive your output. Bring this printed record to the mid-core evaluation. Each student’s log becomes part of the final clerkship evaluation form for the clerkship director to review and include in the final grade.